According to WHO, Diabetes is a chronic, metabolic disease characterized by elevated levels of blood glucose, which leads over time to serious damage to the heart, blood vessels, eyes, kidneys and nerves. Globally, around 387 million persons are affected by this disorder and it is estimated to be more than 640 million by 2040.
Long before advancements in the field of medicine and the eventual unraveling of the disease, its pathogenesis and treatments, the clinical entity was first described in the Egyptian medical papyrus of herbal knowledge, ‘Ebers Papyrus’ (c. 1500 BC). Ayurvedic physicians called it ‘madhumeha’, meaning ‘honey urine’.
Diagnosis:
Prior to the 20th century, diagnosis of diabetes relied solely on clinical observation including symptoms such as polyuria, polydipsia, weight loss, etc. Physicians occasionally even tasted urine to confirm its sweetness. Chemical tests available at the time were done using Benedict’s reagent or Fehling’s solution.
Oral Glucose Tolerance Test (OGTT), was performed for the first time in 1917, which was simplified later in 1963. In the 1980s, Diabetes was classified on the basis of OGTT with 2-time points (fasting and 2-h).
The 21st century saw the advent of HbA1c testing as an emerging diagnostic tool. Today, diagnosis is evidence‐based. Blood tests are standard: a fasting plasma glucose ≥ 126 mg/dL, a 2-hour plasma glucose ≥ 200 mg/dL during a 75 g OGTT, or an HbA₁c ≥ 6.5% are among the established diagnostic criteria.

Treatment:
In the mid1800s, the remedy was considered to be bloodletting and opium. In the 20th century, patients were provided with extra nourishment to compensate for the nutrient losses suffered through urine. This however, resulted in fatalities and it was later found that the contrary i.e. dietary restriction improved the symptoms. Various sugar-free, low-carbohydrate diets gained immense popularity.
After pancreas was incriminated as the focus of the disease, multiple attempts were made at treating diabetes with pancreatic extracts which yielded mixed results.
In 1920, Frederick Banting decided to conduct an experiment by ligating the pancreatic ducts of dogs and keeping them alive till acini degenerated, leaving behind the Islets and isolating the internal secretion to relieve glycosuria. John MacLeod offered him laboratory facilities, dogs, and Charles H Best— a medical student for practical help. Along with James Collip, a biochemist who aided in producing a nontoxic pancreatic extract. In January 1922, The first patient was treated, a fourteen year old boy— Leonard Thompson.
Over the spring of 1922, Best managed to improve his techniques to the point where large quantities of insulin could be extracted on demand, but the preparation remained impure. The drug firm Eli Lilly and Company had offered assistance not long after the first publications in 1921, and they took Lilly up on the offer in April. In November, Lilly’s head chemist, George B. Walden discovered isoelectric precipitation and was able to produce large quantities of highly refined insulin. Shortly thereafter, insulin was offered for sale to the general public.
Insulin was derived from animals (porcine or bovine) which led to allergic reactions in several patients. Patients also lacked the means to properly monitor their sugar levels and adjust insulin accordingly.
The conventional approach of insulin delivery involves the use of needle injections which significantly affects the compliance of patients to insulin use.
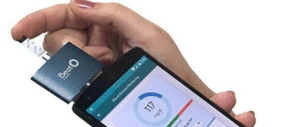
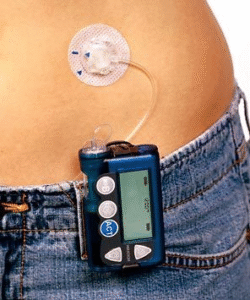
The first genetically engineered, synthetic ‘human’ insulin was produced in 1978 using E. coli. Now, insulin is largely human (via recombinant DNA technology). Delivery devices include disposable syringes, insulin pens, pumps and microcomputer closed‐loop systems (nano pumps) that link continuous glucose monitoring to insulin delivery. Other less invasive means of insulin delivery that involve the use of nanoparticles are also being explored to facilitate insulin delivery orally, transdermally, and/or via inhalation.

Insulin manufacturing plants:
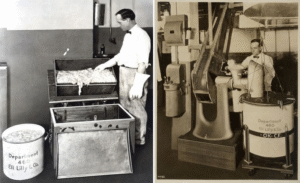
Earlier, commercial insulin production relied on collecting pancreatic glands from slaughterhouses/meat-packing houses. The extraction and purification processes were manual, and flawed. As the demand for insulin grew, supply lagged. The subpar purification process and ensuing adverse reactions drove manufacturers to improve the approach.
Today, insulin production is biotechnology savvy and mass-scale. Recombinant insulin is produced in bacteria or yeast cells, followed by high-throughput purification under strict guidelines. Analogue insulin with altered amino-acid sequences provide tailored pharmacokinetics (rapid-acting, long-acting). Manufacturing plants are global, automated, and capable of meeting worldwide demand.

Diabetic retinopathy:
Several advanced investigation options are available— optical coherence tomography (OCT) and fluorescein angiography which can detect the disease early on. Treatment includes— laser photocoagulation, intravitreal anti-VEGF injections, vitrectomy.
Management of Diabetic foot:
Earlier, poor understanding of the pathophysiology led to poor prognosis and often involved amputations.
Now, entire teams and standalone centres are specialised for appropriate management of diabetic foot. Custom off‐loading footwear, early infection control, vascular assessment, wound care reduce amputation rates.
Pancreatic transplant:
Most pancreatic transplants are performed to treat type 1 diabetes. But it’s usually only for those with serious diabetes complications, because pancreas transplants can have significant side effects.
Stem cell therapy:
In a revolutionary case reported by Wang et al, a 25-year-old woman with type 1 diabetes achieved insulin independence within three months after receiving autologous islet-like cells. The study marks a significant advancement in diabetes treatment. However, it reflects a preliminary success, and long-term studies are required to determine whether insulin independence can be maintained permanently.