
The United Nations General Assembly established March 21 as World Down Syndrome Day for an annual celebration in 2011. The theme for the inaugural observance in 2012 was “Let Us Build an Inclusive Society for All.” Each year features a different theme, and in 2025, it was “Improve Our Support Systems.” The purpose of this special day is to raise awareness that individuals with Down syndrome should have the opportunity to lead fulfilling lives, receiving inclusion on a full and equal basis with others in all areas of society.
The global incidence of Down syndrome is approximately 1 in 1,000 to 1 in 1,100 live births. This figure can fluctuate by region, with an incidence of about 1 in 700 live births in the USA and approximately 1 in 850 live births in India. The condition arises from a genetic abnormality involving an extra chromosome 21 in the genetic structure of affected individuals. Children with Down syndrome exhibit varying degrees of intellectual and cognitive disabilities, along with distinctive facial features and disorders affecting various organ systems in varying proportions, such as the intestines, heart, and blood. A common issue encountered by paediatric surgeons with Down syndrome infants is a condition known as duodenal atresia, which requires surgical intervention during the neonatal period to ensure the patency of the intestinal tract.
The global incidence of detecting Down syndrome in foetuses is on the rise due to several factors, including advancing maternal age. Nevertheless, despite improvements in detection rates, increased terminations have resulted in only a minimal increase in the incidence of live births over the decades. As illustrated in figure 2, the percentage reduction in live births has been steadily increasing, reaching approximately 60% by 2015.
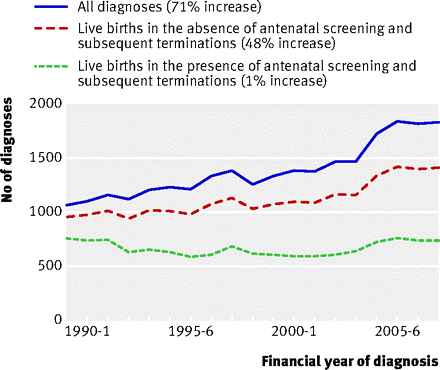
Figure 1: Source: BMJ 2009;339: b3794 (Trends in Down Syndrome Live Births)
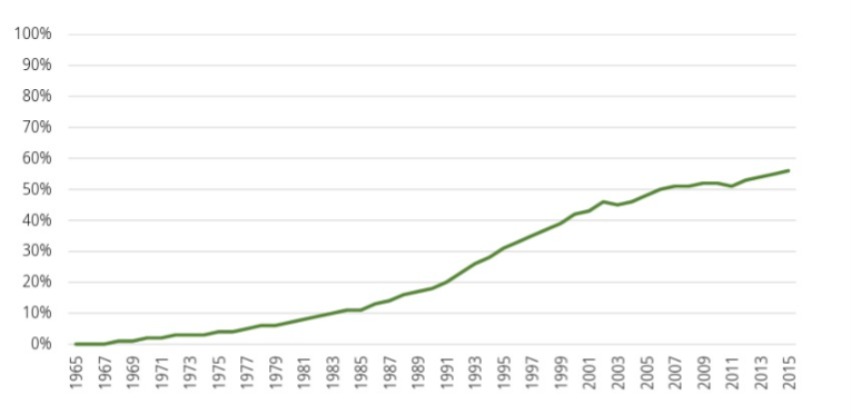
Figure 2: The percentage of live births of babies with Down Syndrome reduced as a result of screening and elective terminations in Europe 1965-2015 (Gert de Graaf, Frank Buckley, and Brian Skotko)
The 2030 UN Agenda for Sustainable Development is a global plan of action for people, planet, and prosperity, pledging that “no one will be left behind”. It aims to ensure that all human beings can fulfil their potential in dignity, equality, and in a healthy environment. Unfortunately, individuals with Down syndrome face various challenges, particularly in education and employment, and their acceptance and integration into society also pose significant difficulties.
A concerning trend is the steady decrease in the number of babies born with Down syndrome. Antenatal screening strategies, both non-invasive and invasive, such as NIPT (Non-invasive Prenatal Testing), blood tests conducted on the pregnant mother (including PAPP-A, β-hCG, AFP, oestradiol, and inhibin-A), ultrasound scans, and amniocentesis followed by genetic analysis, specifically target chromosomal anomalies, including Down syndrome, in foetuses.
Following a diagnosis of Down syndrome, medical counselling typically offers families several options regarding the condition. Ideally, families should have the choice to either continue the pregnancy or opt for termination of the foetus. In an even more ideal scenario, every baby with Down syndrome should be allowed to be born and live a life as normal as anyone else, with any challenges addressed as they arise.
However, this situation is increasingly rare, particularly in an era where the desire for a ‘normal’ baby is becoming more prevalent. In fact, the definition of “acceptable normality” is narrowing, while the definition of “unacceptable abnormalities” is expanding due to advancements in diagnostic methods. The challenges associated with raising a potentially physically and intellectually challenged child are unlikely to encourage any family, regardless of wealth or background, in either the Western or Eastern worlds.
Unfortunately, the medical fraternity often demonstrates a bias towards terminating affected foetuses, and these biases frequently influence the counselling process. Many families feel pressured to comply, perceiving themselves as inadequate for raising an ‘abnormal’ baby due to financial, social, or other concerns. While the medical profession aims to act in the best interests of the family, the procedure raises complex moral and ethical questions. On one hand, state and medical bodies strive to elevate the Down syndrome population to the same level as the rest of society in terms of education, employment, and the pursuit of happiness. On the other hand, efforts are being made to prevent these individuals from being born in the first place.
Some countries, such as Iceland, have achieved a 100% elimination rate for Down syndrome. In most countries, screening strategies nearly always lead to a reduction in Down syndrome live births. Nevertheless, the overall prevalence of Down syndrome live births remains stable, owing to a lack of access to or refusal of screening strategies. In some rare instances, mothers may choose not to undergo an abortion. This near-total elimination in certain countries has led one author to aptly describe this phenomenon as a ‘search-and-destroy’ technology.
The issue of termination, which relates not only to Down syndrome but also various foetal conditions, presents numerous ethical conundrums. Generally, there is little controversy when the mother’s life is at risk. Typically, decisions are driven by rational-economic considerations, where the birth of the baby could significantly affect the social, economic, and psychological well-being of the mother, her immediate family, and society at large.
The rational economic perspective raises troubling questions regarding female foeticide. The ethical justification for aborting a baby diagnosed with Down syndrome (or any other malformation) due to the perceived burden on the family is unclear, as the same rationale could be applied to a female child, potentially disrupting the social lives of some mothers. Some ethicists contend that there may be no distinction between female infanticide and the termination of a pregnancy due to Down syndrome.
In medical ethics, the dichotomy of “life or no life” is never a valid option. However, in the field of foetal medicine, terminating pregnancy is often viewed as a viable alternative. Frequently, it is impossible to address the disease without also terminating the pregnancy. The general principle in medicine is to diagnose a condition with the intent to either treat it or to refrain from intervention if no treatment is possible or available. One does not eliminate the patient when the disease is untreatable.
At present, the perceived “viability” of the baby significantly influences decisions regarding termination. The definition of survivability has shifted from 28 weeks to 24 weeks due to advancements in neonatal care. This evolution raises further ethical questions, suggesting that ethical considerations may shift in response to technological advancements, which presents a contentious aspect of ethics. Ultimately, despite the myriad conundrums surrounding the issue of termination, the decision-making process often reflects the perspectives of the family and society.
However, what are the views of those affected by Down syndrome themselves? The challenge within the complex ethics of foetal medicine lies in the fact that one party in this equation—the foetus—has no voice, while the other party, the mother, is vocal about her rights and responsibilities. There are several studies that measure how children with Down syndrome perceive their lives. One such study indicates that they can express profound love and contentment towards their families and society, despite varying levels of intellectual impairment.
A small study involving 284 children with Down syndrome aged over 12, titled ‘Self-perceptions from People with Down Syndrome’ (Skotko, Levine, and Goldstein, American Journal of Medical Genetics, 2011), revealed that nearly 99% of participants reported being happy with their lives, 97% liked who they are, and 96% liked their appearance. Almost all participants expressed love for their families, and 97% liked their siblings. While 86% felt they could make friends easily, those facing challenges often experienced isolating living situations. Only a small percentage expressed sadness about their lives, despite the overwhelming majority indicating a joyful and fulfilling existence.
This study raises troubling questions regarding society’s inclination to terminate pregnancies following a diagnosis of Down syndrome. In an ideal society, a diagnosis would serve only to prepare parents and society for the arrival of the baby. However, when faced with a prenatal diagnosis of Down syndrome, the ethical, moral, legal, medical, and social dimensions become far more complex than they may initially appear. The moral and ethical issues surrounding foetal medicine and the management of non-treatable conditions, such as Down syndrome—often a prototypical example—are likely to become more pronounced in the future as more diseases fall within the realm of predelivery diagnoses.
A Greek myth depicts the casting of deformed children off a cliff, while only the normal ones receive care. This notion of survival of the fittest has manifested itself in a modern context through the termination of unborn foetuses. There are perhaps no definitive right or wrong answers to these issues. One perspective questions whether a society that does not embrace any abnormalities outside its definition of normalcy can be considered truly healthy. Another posits that the maturity of a society is measured by how it treats its members who may not contribute in conventional ways—the handicapped, the elderly, the ill, and even animals deemed useless. How does modernity, combined with the ever-increasing technological advancements in medicine, navigate these complex issues? The future promises to be intriguing.




